|
| Patient: 55 year old male |
| History: 55 year old male with SVC syndrome from lung cancer who is experiencing hypoxemia. We are asked to evaluate for pulmonary embolus. |
Image Size:
|
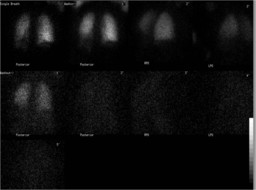
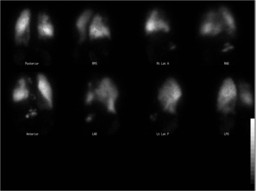
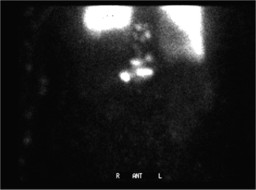
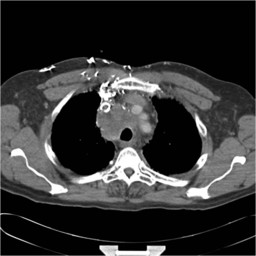
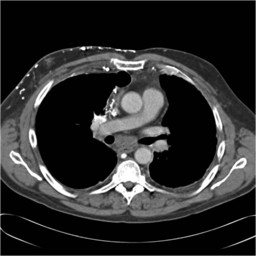
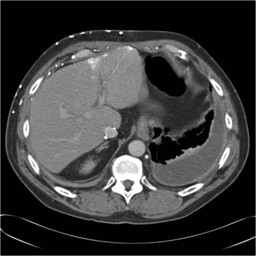
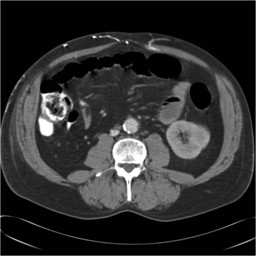
| Findings: The xenon-133 ventilation images show hypoventilation to the left lung base on single breath and wash-in images. There is no abnormal Xe-133 retention during the washout phase. The flow images of the perfusion study demonstrate extensive venous collateralization due to the patient's known SVC obstruction. The perfusion images show a moderate sized perfusion defect in the right anterior and superior lung as well as hypoperfusion at the left base, the latter corresponding to the ventilation abnormality described above. Radiotracer activity is noted in the mediastinum and in the epigastrium, consistent with tracer uptake in the area of the patient's known mediastinal tumor as well as the quadrate lobe of the liver due to extensive collaterals from SVC obstruction. Activity in the kidneys, stomach and spleen is evidence of a right to left shunt. CT: Large right paratracheal mass with interval growth resulting in superior vena cava obstruction. Filling defects seen in the superior vena cava is probably direct invasion of the vein by tumor. As a result of this severe obstruction systemic-to-pulmonary venovenous collateral flow have formed in addition to multiple right chest wall collateral veins resulting in a "hot quadrate" sign in the left hepatic lobe. |
| Diagnosis: SVC syndrome.Ā Right to left shunt. Opinion (for PE): 1. Intermediate likelihood ratio of pulmonary embolism due to a single moderate sized VP mismatch in the right superior and anterior lung. Alternatively this mismatch may also be due to obstruction of pulmonary blood flow from the patient's known mediastinal mass. 2. Matched ventilation perfusion abnormality in the left lower lung corresponding to a left-sided pleural effusion. 3. Right to left shunt which may be contributing to the patient's hypoxia. |
| References: Thank you to Sara Rohr, M.D. for contributing this case. (1) Cihangiroglu et al. Collateral Pathways in Superior Vena Caval Obstruction as Seen on CT. Journal of Computer Assisted Tomography: Volume 25(1) January/February 2001 pp 1-8 (2) Win et al. Superior Vena Cava Obstruction as Suggested by Extrapulmonary Uptake on Lung Scintigraphy. Clinical Nuclear Medicine. 31(2):99-100, February 2006. (3) Nguyen et al. Superior Vena Cava Obstruction with Intrahepatic and Systemic-Pulmonary Venous Right-to-Left Shunts. Clinical Nuclear Medicine. 29(8):491-493, August 2004. |
| Comments: No comments posted. |
| Additional Details:
Case Number: 131111 The reader is fully responsible for confirming the accuracy of this content. |