|
| Patient: 39 year old male |
| History: with left ureteropelvic junction obstruction, status post pyeloplasty and stent placement. Stent was removed 10 weeks ago. |
Image Size:
|
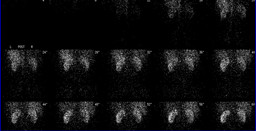
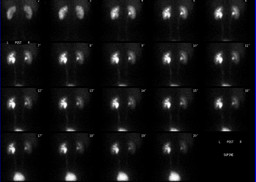
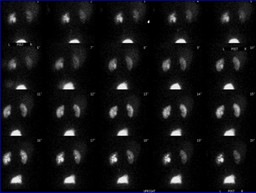
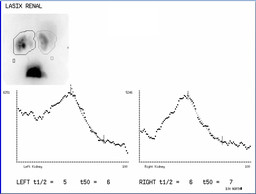
| Findings: RADIOPHARMACEUTICAL: 7.5 mCi Tc-99m MAG 3 i.v. and 40 mg furosemide i.v. FINDINGS: The posterior abdominal radionuclide angiogram demonstrates normal, symmetrical perfusion of the kidneys. The kidneys are normal in size and morphology. There is prompt uptake and excretion of the radiopharmaceutical by both kidneys. There is mild retained activity in the left collecting system, which is mildly dilated. This retained activity persisted after erect positioning. To evaluate for obstruction, the patient was given 40 mg furosemide via slow intravenous injection approximately 30 minutes after the start of the examination. Sequential images were obtained for an additional 20 minutes. Initially, there was slight clearance of tracer activity bilaterally. However, approximately 3 minutes after administration of the diuretic, there is increasing accumulation of tracer activity within the kidneys bilaterally.� Subsquently, there is decreasing activity in both kidney regions. (see lasix graph) |
| Diagnosis: Vasovagal response after diuretic administration. |
| Specific Discussion: Hypotension can be a cause of a false-positive diuretic renal study. Adequate hydration is important, with additional fluids as needed if the patient becomes hypotensive. |
| References: aafp.org/afp/20010515/tips/7.html |
| Comments: No comments posted. |
| Additional Details:
Case Number: 125447 The reader is fully responsible for confirming the accuracy of this content. |