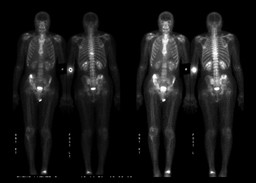
| Findings: RADIOPHARMACEUTICAL: 33 mCi Tc-99m MDP i.v.
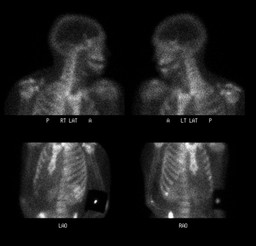
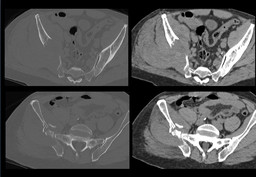
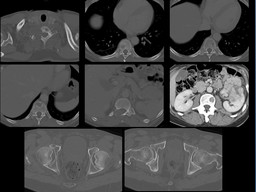
FINDINGS: There is increased activity within the approximately T9 vertebral body, which corresponds with a lytic lesion with pathologic fracture seen on CT examination. There is also increased uptake within the right ilium, corresponding with the large lytic lesion with pathologic fracture. Of note, there are numerous other lytic metastases throughout the thoracolumbar spine and pelvis seen on CT which demonstrate no scintigraphic correlate.
A focus of increased uptake in the distal left tibia is most consistent with the history of left ankle fracture which the patient reports occurred 9 years ago. Mild uptake in the bilateral shoulders and the right knee are consistent with degenerative joint disease. Incidental note is made of partial extravasation at the injection site, with overlying lead shield. |