| Findings: RADIOPHARMACEUTICAL: 21.54 mCi Tc-99m MDP i.v.
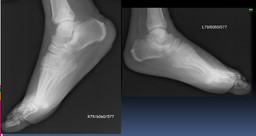
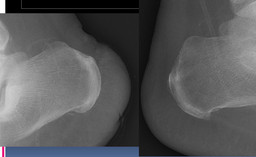
FINDINGS: Triple phase examination of the feet was performed consisting of radionuclide angiography, immediate post-injection images, and delayed images. Angiography demonstrates increased flow to the right heel. There is markedly decreased flow to the left foot with minimal flow evident only at the level of the proximal tibia. The immediate postinjection images demonstrate increased uptake in the region of the calcaneus and overlying soft tissues.
5 hour-delayed images demonstrate increased activity within the calcaneus with slight remaing overlying soft-tissue uptake, and 24 hour delayed images (after soft-tissue clearance) confirm abnormally increased uptake in the calcaneus. Increased activity is also noted within the right ankle joint and midfoot in the delayed images. Immediate static images as well as the 5-hour delayed images demonstrate markedly decreased activity within the left foot with complete absence activity beyond the level of the left midfoot. These findings persist on the 24-hour delayed images. |