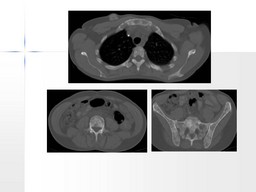
General Discussion: For bone marrow metastases, overall sensitivity of PET and bone scan is comparable, but PET has superior specificity.FDG PET is superior to bone scan for detecting osteolytic metastases but is inferior for visualizing osteoblastic metastases. FDG PET cannot replace bone scan for detection of bone metastases in breast cancer. Patients with more aggressive tumors may benefit more from PET given the high likelihood of osteolytic bone metastases with those malignancies.
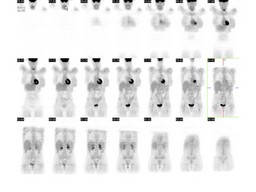
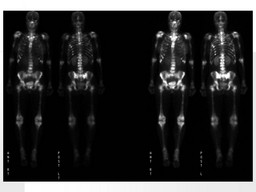
99 mTc-MDP shows the osteoblastic bone reaction to tumor infiltration, 18F-FDG measures glucose uptake into the tumor itself. This, along iwith is better resolution, allows PET to detect small volumes of disease before a secondary cortical bone reaction appears. In a series of 25 patients with bone metastases (16 secondary to breast cancer and nine secondary to lung cancer) in whom both BS and PET procedures were performed before and after chemotherapy, BS and PET showed discordant results in five patients (20%) . These five patients showed improvement on PET examinations over time, with a reduction in FDG uptake and/or in the number of lesions detected. In three of them, BS suggested progression of metastatic disease and in the remaining two, results on serial BS remained unchanged. Clinical follow-up, serial tumor marker levels and radiological confirmation supported the PET findings. Therefore, in this preliminary experience, serial PET studies seemed more accurate than serial BS in treatment control of patients with bone metastases, in both types of primary tumor. It is important to know the danger of misinterpretation of BS due to the flare phenomenon and a persistent bone reaction lasting for more than 6–12 months after chemotherapy.