General Discussion: 39-year-old African-American gentleman with a history
significant for nephrolithiasis, status post lithotripsy in several years ago, moderate
persistent asthma, hypertension, and hypercholesterolemia, who presented to the
Barnes-Jewish Hospital Emergency Department with a complaint of diffuse body cramps, 10 out of 10 in severity, right jaw
pain, left arm pain, lightheadedness and sweating that developed after working
outside as a mover for approximately two hours. He states it was extremely hot
outside and humid, and he was drinking two to three cups of water, as well as
one large container of soda; however, after approximately two hours, he began
sweating profusely and developed muscle pain and spasms all over his body,
including his jaw and shoulders. In addition, he noted lightheadedness and
some exacerbation of his shortness of breath, along with some nausea and one
episode of vomiting.
On admission, the patient was found to have elevated CK to 3931, increasing to
11,015 over the next day. The patient was started on aggressive IV hydration
with alkalinized fluids to protect his kidneys from pigment-induced ATN. His
renal function as well as electrolytes and uric acid levels were monitored.
His CK continued to increase peaking at 31,100 before declining to 5930
on the day of discharge.
The patient's renal function remained stable throughout his hospitalization.
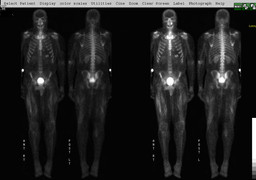
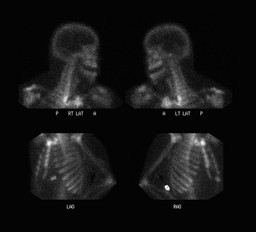
The patient's muscle cramps improved. The patient underwent a bone scan which showed increased uptake especially in the large muscles of both
legs. This finding is consistent with rhabdomyolysis and could be indicative
of exercise-induced rhabdomyolysis but does not rule out metabolic myopathy. A muscle biopsy was advised to exclude the latter.